
|
|||
|---|---|---|---|
|
|
Sixtieen years of application of the intensive multifactorial neurorehabilitation system at CIREN |
|
|
|
Institution: Internacional Center of Neurological Restoration - CIREN (Cuba) |
Armando Sentmanat Belison Coralina Martinez Hidalgo sentmanat@neuro.ciren.cu |
|
|
|
|
|||
|
|
http://www.efdeportes.com/ Revista Digital - Buenos Aires - Año 10 - N° 93 - Febrero de 2006 |
|
|
1 / 1
Introduction
The International Center of Neurologic Restoration (CIREN) was inaugurated on February 26th, 1989. At this center, a group of professionals in the fields of neurosurgery and the neurosciences planned the application of state-of-the-art surgical techniques of minimal access for the treatment of Parkinson's Disease. Therefore simultaneous to the surgical practice, the patient's rehabilitation process submitted to surgery was thus started by a group of professionals, including professors in physical culture, speech therapists, occupational therapists, kinesiologists, physicians and nurses.
After results were obtained from these first experiences, a pre-surgical period of general -type preparation was included in these issues- in the case of patients that would undergo a surgical intervention for them to assimilate much quicker the process of post-surgical rehabilitation. Practical results were obtained with the pre-surgical - rehabilitation combination - general preparation and post-surgical rehabilitation, which widened the center's scopes and thus the spectrum of attention to the patients with other neurological diseases increased. The process of rehabilitation was developed based fundamentally in previous studies performed on the plasticity of the nervous system and also on some knowledge of the Cardinal Principles of Neurorehabilitation described by J.C. Moore in 1972[1]. Dr. Rafael Estrada referred to these studies in his book entitled "Neuroplasticity" in 1988[2] taken from criteria by Dr. Paul Bach-Rita in his work entitled "Cerebral Mechanisms of Brain Substitution"[3] and his own criteria on the mechanisms of neuroplasticity.
The development of the rehabilitation program and positive results achieved with time, defined the problem of how to scientifically and methodologically establish the Neurological Rehabilitation Model called Intensive Multifactorial Neurorehabilitation System (IMNS). As an initial step to face this problem, the preparation of programs for rehabilitation treatments was on its way according to specialties for each disease and following corresponding methodological orientations for its application. A bibliographic revision on the plasticity of the Central Nervous System (CNS) was carried out for the documentation of the Intensive Multifactorial Neurorehabilitation System (IMNS). In the study of the literature on neuroplasticity, Dr. Bergado - a Cuban reseacher - emphasiged Dr. Francisco Ramón y Cajal´s most severe assertion at the end of the eighteenth century in this work entitled "Degeneration and Regeneration of the Nervous System" where he remarked...'that the functional specialization of the brain imposes two great gasps on the neurons, that is: incapacity for the proliferation and irreversibility of the intraprotoplasmatic differentiation, for in adult brains, nervous vias are something fixed, terminated and unchangeable. All dies and nothing can be regenetated'. But nevertheless, with the expertise that caharacterized Dr. Cajal, he added these words to the same paragraph; ..."it corresponds to future science to change, if possible, this unkind remark.."[4].
It was also necessary to revise and deeply study the international literature on the mechanisma of neuroplasticity, introduced in Cuba by Dr. Paul Bach-Rita in works conducted on cerebral plasticity and brain machanisms of sensory substitution. Dr. Rafael Estrada as Director of the National Institute of Neurology and Neurosurgery used these issues successfully and made contributions of his own with collaborators in the 80's. Young and Delwade's works[5] in the 90's and most recently, the revision and contribution of cuban scientists Drs. Jorge Bergado and William Almaguer - CIREN's researchers - based on the cellular mechanisms of neuroplasticity were carried out. Both scientists have researched on one of the scientific bases fundamental to sustain the Intesive Multifactorial Neurorehabilitation System.
The Cardinal Principles of Rehabilitation were revised and analyzed, considering the experiences described by Professor J.C. Moore, as she estudied the basic features for the systematic performance of professionals in the field of neurologic rehabilitation; therefore, these features were later adopted as well as other fundamental bases for IMNS. The bibliographic investigation also included studies on physical exercises with therapeutic aims - that comprised studies from 2000 BC up to de modern age.
The principal models of neurologic rehabilitation were also analyzed taking as models the works by Licht[6], Kottke and collaborators[7] on the therapy of exercising. Daniel's and Worthingham's criteria on brain muscle interaction and the importance to assess the muscular function before and after the patient's rehabilitation[4] were also considered. The studies by Crossman[9] and Rabbit[10] in two different epochs, gave great importance to exercise repetition to establish movement patterns.
In order to know the world status on rehabilitation, the methods of neurologic rehabilitation internationally used in tha past and present century could not go without study. Among these Kenny's[11], Bobath[12], Kabat-Knott-Voss[13] and Votja's[14] methods were the most used by health institutions and independent professionals during the twentieth century and part of the present. Brumnstrom, Frenkel, Rood[15], Pilates[16] and Felderkrais methods[17], have also influenced on the development of neurologic rehabilitation in contemporary times. All these methods have physical exercising as a common denominator and its systematic repetition as a fundamental way to achieve in those patients with neurological diseases, the learning or re-learning of movement patterns, the recovery of physical capacities affected by such diseases, improving of postures and normalization of the muscular tone[15].
The Intensive Multifactorial Neurorrehabilitation System is an "ecclectic" model[18], based on all positive elements of different models, methods, procedures, techniques and specialties within neurological rehabilitation. Also special pedagogy and physical culture according to each patients needs, make this treatment come closer to the so-called Alternative Medicine. As to Alternative Medicine, IMNS uses acupuncture, Bach´s floral therapy, homeopathy, exercising and techniques of Chinese Traditional Medicine. Laser puncture, magnetotherapy and ozonotherapy among other therapeutic alternatives combined with methods amd techniques from western medicine are also used.
The intensive physical work that characterizes IMNS with a 7-daily-hour treatment for each person in an individualized way, is methodologically organized and adequately dosified according to its general program and such specific programs for each discipline. This program is much more closer as a whole to the characteristics in the training of sportsmen - fundamentally applied by those licensed in physical culture within this pedagogical profile. For this motive, the bibliographic analysis included theorics of sports training internationally described by Harre, Matveev, Ozolin and others and also the one described by the Cuban Professor Armando Forteza. All issues were included in the revision of his "Methodological Bases of Sports Training"[9] with arguments of the General Principles of Sports Training[9] - a modified theory for its closeness in the formation of professionals of physical culture. The personnel who have long been applying this form of teaching for the physical rehabilitation process - developed at CIREN - have adopted it as bases to support IMNS.
Other aspects revised in the international literature were the contemporary criteria on multi, inter and transdisciplinary rehabilitation. Many worldwide institutions have a staff formed by specialists in different disciplines, but in daily practice, there is not such an efficient coordination among them, as well as a unique direction to join efforts and individualized criteria to offer each patient an integral and personalized attention. Other institutions do not have these teamworks and many professionals in medicine and rehabilitation dedicate themselves to the private and unipersonal attention of patients[6].
Restrepo and Lugo in their "Rehabilitation in Health"(1995), affirm that the integration of an interdisciplinary team constitutes the bases for a good assistential academic program, also the work in teams must be performed with the best possible relationship among its members, as all must participate and profit from the contribution of others[15]. In the work of teams, its members must have specific functions within each group, as well as others that are the result of the group dynamics - elements taken as bases to establish the Interdisciplinary Coordinated Teamwork that characterizes IMNS.
General conception of the intensive multifactorial neurorehabilitation systemNeurologic Restoration arises from the evidence that the Nervous System has neuroplastic and regenerating properties determined by the high differentiation that does not allow neuroplastic cells to reproduce themselves. In compensation Nature chooses the atternative way to give the Nervous System the capacity for a superior repairment, which is much more complex than the rest of the tissues- a fact demonstrated by performed experimental evidences. It was inferred from the analyses by experts of reference, that from a mathematical point of view and accumulated practical experience for so many years in the patients' neurological rehabilitation developed at CIREN - many long periods of time were thus needed to achieve the pretended level of exercising.
A preliminary conclusion was, that it was only possible to obtain similar results in less time if a form of treatment with a systematic frequency based on many hour - session trainning was applied with an optimum use of the time, by adequately applying exercising techniques, in reference to the patient's sequels, characteristics of the patient's general status and an efficient supervision and systematic evolution.
Expressed in other way, in order to perform such a high volume of physical activity, a great amount of time is needed that can only be achieved in a less period of time, when rehabilitation procedures with an intensive character are strictly controlled and performed.
Although it is a fact that natural recovery may also occur, attempts are made to improve and accelerate this process. Many health areas have developed treatments without a clear understanding on its functioning, and it is not really known whether the method is good at all or not. The rehabilitation of lesions of the Central Nervous System is not an exception, although some therapeutic techniques are based on clear theorical considerations[6]. In the theorical and practical accumulated experience applying the Intensive Multifactorial Neurorehabilitation System for 16 years, it was concluded that the physical therapist should not use one method in particular, but the one according to each patient's specific characteristics, he/she must choose the most convenient method or most convenient combination of methods.
All the criteria previously mentioned, made possible to formulate the concept of Intensive Multifactorial Neurorehabilitation System, defined as "a model aimed at rehabilitation. "This method must be used with a systemic approach, in an integral and systematized way combining intensively and adequately dosified form the methods, procedures and therapeutic techniques that make possible a better recovery. This is expected to be carried out in the least possible time and providing the patient with a better quality of life"[18].
The philosophy and scopes of the Intensive Multifactorial Neurorrehabilitation System - as an integral part of the Neurologic Restoration Program at the International Center of Neurologic Restoration (CIREN) - are conditioned by the directing philosophy of this institution, expressed as to its scopes and strategic objectives used in all its levels. On this bases and in correspondence with CIREN'S functions and structure, the activities for the interdisciplinary integration of processes of neurologic restoration leading to the establishment of programs for the intensive personalized care, are thus developed with special attention according to each patient's needs.
CIREN'S researchers have demonstrated that with the application of neurorestorative methods, significant results can be obtained in the improvement of altered neurologic functions, by submitting the patient to an intensive regulated physical activity within the context of multifactorial treatment programs. IMNS proposal was conformed on the basis of compatibility of four essential factors: mechanisms of neuroplasticity, the cardinal principles of rehabilitation, general principles of sports training of the Cuban School and coordinated work within an interdisciplinary teamwork that together, give the intensive character necessary to each patient's program.
Some resultsRecent studies with transcranial magnetic stimulation(TMS) describe bilateral cortical changes in patients with unique unilateral vascular lesions. It also constitutes a frequent finding in the EEG. Following are illustrated images taken with High Frequency Transcranial Magnetic Stimulation to determine the brain mapping at the beginning and end of treatment. This sample was performed on a 49- year- old patient with a diagnosis of Stroke in the left hemisphere with a 4-year- and 9 moths evolution, bearer of a right hemiparesia before and after his submission to IMNS treatment.
Images belong to a sample case of study "Effects of the Application of a Neurologic Restoration Program", as a pattern for the activation of neuroplasticity to recover lost motor functions. Presentation of cases[20] were conducted by CIREN'S researchers, Sánchez B, Gómez L, Torres M, and Sentmanat A.(Figs 1, 2).
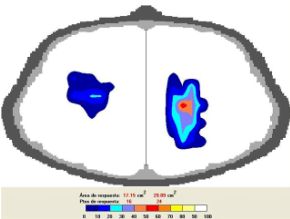
Fig. 1 Behavior of brain hemispheres through evaluation with
Trascranial Magnetic Stimulation before the application
of treatment.
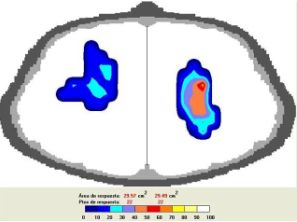
Fig. 2 Behaivor of brain hemispheres after the
treatment was over. One can observe the
increase of activity in the affected hemisphere
and reorganization of the healthy one, a fact
attributed to the stimulation received through
IMNS.
When rehabilitation actions are organized in an integral way by joining all links that the development of knowledge offers on biologic and psycho-social phenomena, important advance in the rehabilitation of functions and an adequate interaction between patient and physical therapist can thus be achieved. The rehabilitation time dedicated to each patient within the IMNS, can amount to 38,5 hours, on the bases of 7 - daily hours, divided in two sessions of 3,5 hours each from Monday thru Friday and a 3,5 hour session - on Saturdays. Fundamentally, the time dedicated to the physical activity, plus the volume and intensity of exercising - which is high - and the pedagogical character implicit in the rehabilitation process - reinforced by those licensed in physical culture, as well as occupational and speech therapists with a pedagogical formation, resemble that of IMNS as to the sports training with therapeutic aims.
By keeping in mind the training principles when organizing, planning, performing and assessing the intensive neurorehabilitation process, it guarantees the effectiveness of the treatment that has a direct bearing on the patient's positive evolution.
The acquired experience from 16 years of application, allows to affirm that human resources are the most important ones for the good development of rehabilitation process. Equipment and auxiliary means have a determined level of importance in the development of this process, but the specialists and their guidance as well as their knowledge, expertise and above all, their creativity - is a fact that makes them irreplaceable.
During the 16 years of the IMNS application at CIREN, more than 16,000 patients of more than 70 countries have been assisted. The statistical behavior is shown in the attention to patients and hours administered for each specialty during 2000 - 2004(Table 1 and 2).
Table 1.
Assisted patients with IMNS between 2000 y 2004.
Table 2.
Hours of administered treatments to patients withl IMNS during 2000 y 2004.
In the Tables, the General IMNS Statistics is resumed as to assisted patients, time of administered treatment from five basic specialties: Physical Exercises, Occupational Therapy, Speech Therapy, Physiotherapy and Psychomotor Integral Evaluation applied at the Psychomotor Integral Evaluation Laboratory that gives evidence of a significcal growth in the last two years, in reference to the accumulated experience by CIREN'S specialists with the application of the System since 1989.
Conclusions
-
New knowlodge has been supplied for the introduccion of a New Cuban Model of Neurologic Restoration.
-
A new scientific-methodological conception was introduced for the application of rehabilitation treatments of an intensive character.
-
The effectiveness of the work was assessed within an interdisciplinary team to approach the rehabilitation of patients bearers of chronic neurological diseases.
-
The application of the principles of sports treatment adopted into the rehabilitation process was thus assessed. It seems to modulate in an effective way the stimulation to neuroplastic mechanisms and it accelerates the patients' recovery of lost functions.
-
It was possible to improve the quality of life of more than 16,000 persons affected by sequels of neurological diseases submitted to IMNS from more than 70 countries, where Cuba is considered as principal emissor.
References
-
Moore J. Neuroanatomical Considerations Relating to Recovery of Function: Theoretical Considerations for brain injury Rehabilitation. Verlag: Ed Bach y Rita Hans Huber, Publishers; 1980 p. 9-90.
-
Estrada R. Neuroplasticidad. La Habana: Instituto de Neurología y Neurocirugía; 1988. p. 32-65.
-
Bach-Rita P. Mecanismos cerebrales de la sustitución sensorial. México: Trillas; 1979. p. 365.
-
Bergado JA, Almaguer W. Mecanismos celulares de la Neuroplasticidad. Rev. Neurol 2002;31(11)1074-95.
-
Young RR, Delwade PI. Principles and Practice of Restorative Neurology. Oxford: Butterworth-Heinemann; 1992. p. 345-352.
-
Licht S. Terapéutica por el ejercicio. La Habana: Edición Revolucionaria; 1963. p. 104-110.
-
Kottke FJ, Stillwell GK, Lehmann JF. Krusen. Medicina Física y Rehabilitación. Buenos Aires: Panamericana; 1990. p. 54-127.
-
Worthingham C. Pruebas funcionales musculares. México: Interamericana; 1973.
-
Crossman ERFV. Theory of acquisition of speed-skill. Ergonomics, 1959; 2: 153-6.
-
Rabbit PMA. Sequential reactions to holding. En Holding DH. Human Skills. Chichester (England): John Wiley and Sons. 1981; 153-4.
-
Viel E. El Método Kabat. Facilitación neuromuscular propioceptiva . Barcelona; 1994: Masson. p. 17-26.
-
Bobath B, Bobath K. Desarrollo motor en distintos tipos de parálisis cerebral. Buenos Aires: Panamericana; 1992.
-
Voss DE, Ionta MK, Myers BJ. Facilitación Neuromuscular Propioceptiva. Buenos Aires; 1987: Médica Panamericana. p. 19-25.
-
Sánchez de Muniain P, Pardo P, Varela E, Del Pino E. La locomoción refleja de Vojta como principio terapéutico. Rehabilitación(Madr) 1997; 31: 440-447.
-
Restrepo R, Lugo LH. Rehabilitación en salud. Una mirada necesaria. Medellín:Ed. Universitaria de Antioquia; 1995. p. 217- 220.
-
Cuva AM. Método Pilates. www.studio.pilates.it/joseph_pilates; 2002 (1 pantalla).
-
Feldenkrais M. Autoconciencia por el Movimiento. Barcelona; 1997: Ed. Paidós Ibérica. p. 93.
-
Sentmanat A. De vuelta a la vida. Sistema de Neurorrehabilitación Multifactorial Intensiva. Sangova, S.A. Madrid, 2003. p.1-187.
-
Forteza A, Ranzola A. Bases del Entrenamiento Deportivo. La Habana: Ciencia y Técnica; 1988. p. 26-36
-
Sánchez B, Gómez L, Torres M, Sentmanat A. Efectos de la aplicación de un programa de Restauración Neurológica como patrón de activación de la neuroplasticidad para recuperar funciones motoras. Presentación de un caso. 2004; Digital (6 pantallas).
| |
|
|---|---|
|
revista
digital · Año 10 · N° 93 | Buenos Aires, Febrero 2006 |
|